
The following article by James Linney, first posted by Weekly Worker, shows the dismal inability to defeat the pandemic points to a wider systemic failure.
COVID-19 – NOT GOING AWAY
Last week the total number of deaths in the UK relating to Covid-19 surpassed 200,000 – a truly horrible statistic and a far cry from the less than 20,000 deaths that the government’s chief scientific advisor, Patrick Vallance, said would be a good outcome from the pandemic.
Of course, Vallance made this statement near the beginning of the pandemic in March 2020 and in the two and a half years since we have learnt much about the virus, SARS-CoV-2: in the early pre-vaccination year we sadly witnessed how deadly it could be (100,000 of the deaths in the UK were in the first 12 months) and in the past year we have seen how, despite the available vaccinations, which thankfully have reduced the death rate, SARS-CoV-2 has a tendency to repeatedly mutate and continues to prodigiously infect people globally.
Tragically, despite our experience, some people – the UK government included – seem unable or unwilling to learn the most basic public health lessons. The Johnson administration did not even seem aware of the most basic rule, which has been well known way before Edward Jenner started inoculating people from smallpox over 200 years ago: namely that allowing people to become infected with a potentially deadly pathogen to create herd immunity is hare-brained. We will never know exactly how many of the 200,000 deaths could have easily been prevented if these lessons had been heeded, but they amount to tens of thousands for sure.
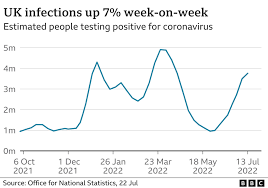
The story of the pandemic is far from over, and the UK is currently seeing a week-on-week increase in the number of cases and – worryingly – hospitalisations too. The latest Office for National Statistics figures predict that as of July 5 about 3.5 million people are infected in the UK (a 30% rise on the previous week) – about one in 18 people.1 Hospitalisations of Covid-positive patients also continue to rise, nearing 2,000 per day, and the majority of these (63%) are being treated primarily for a non-Covid condition.
Some people claim this means the seriousness of Covid-19 is being exaggerated, but this is not the case. If, for example, someone is admitted to hospital with a serious infection, heart attack or stroke and has a concurrent Covid-19 infection, the result can be devastating, resulting at least in a much longer recovery, meaning hospital beds stay occupied for longer – and, of course, they also risk infecting other vulnerable patients or staff. Daily deaths from Covid-19 thankfully remain low (less than 100 per day), but there is always a lag of a few weeks in the rise in deaths due to the time it takes people to get seriously ill after first being infected, so rates are likely to rise in the coming weeks.
The current surge in cases is due to the latest variants: BA.4 and BA.5. These first turned up in South Africa in April this year, and they are actually one of several sub-variants of the original Omicron, first recognised by the World Health Organisation back in November 2021; Omicron is now the dominant variant globally and it is itself only one in a long list of Covid-19 variants that have caused worldwide spikes in infection (previous notable variants being alpha and delta).
We are still in very early days when it comes to understanding the implications of this extremely high level of transmissibility on our populations, but there is already another, even more infectious, Omicron variant in the air: BA.2.75, the so called ‘Centaurus’ virus.
Early data on this newest sub-variant, which was first recorded in India but now has spread globally including having arrived in the UK, suggests it may have an R0 (rate of infection) greater than 18: this would make it one of the most contagious viruses on earth. Most worryingly this sub-variant has 12 unique mutations on the outer protein surface, compared to the one or two of most variants, which makes it a bit of a wild card; the more mutations, the greater the possibility that it may avoid detection by our immune systems.
What next?
It is too early to predict what impact this new sub-variant will have, but there is a good chance it will be responsible for infection spikes in the near future. As the pandemic progresses, predictions of a variant’s severity and impact become more difficult, because they are complicated by multiple factors, including personal immunity imprints, which can vary from person to person, and other population factors (for example, average age, prevalence of certain co-morbidities or rates of malnutrition). On an individual level the likelihood of being infected and becoming seriously unwell due to future variants such as BA.2.75 will depend on which (if any) previous variants you have recovered from, which combination of vaccinations you have had and how long it has been since your last vaccination or booster. Immunity against the newer Omicron starts to wane after a few months, which is why we are seeing people being infected multiple times.
Turning once again to the UK, despite the unpredictable nature of the pandemic, there are some things we can say with some confidence. Firstly, come September, we will be in the grip of another wave of infections – if not a result of BA.2.75, then another, as yet unknown, variant: and, secondly, the government’s response will be pathetically inadequate then, as it has been throughout.
This winter looks as though it could be particularly challenging for the national health service, because, as currently in evidence in Australia, there is a severe flu virus outbreak this year for the first time since the pandemic started. That is worrying news, given that the NHS is already on its knees; waiting lists for elective treatment, accident and emergency waiting times and ambulance response times are all at record highs and are continuing to worsen month on month.
The looming disaster this autumn/winter and the continued threat of Covid-19 generally does not seem to be concerning our government too much. The message is clear: it considers the pandemic to be essentially over and we are on our own. No attempts are being made to improve ventilation in workplaces or schools, no support is being offered for infected workers to remain at home. There is no community testing, allowing the authorities to keep track and limit the spread of new variants; no imposition of mask-wearing in high-risk environments such as public transport; no serious attempt to properly fund and staff the NHS, so as to be able to deal with future waves.
The Tories are, of course, currently too busy choosing a new leader to bother with any of that and neither of the candidates, as far as I know, has had anything to say about the future threat of Covid or has criticised the way it has been handled under Boris Johnson’s leadership. I am confident that, if asked, both the leadership candidates would echo Johnson’s claim that they “got all the big calls right” during the pandemic – a claim so absurd that it can only be interpreted as an open expression of arrogant disdain for the suffering of anyone not a member of their despicable ruling elite, which takes as a given their privilege to use the pandemic as an opportunity to enable themselves, their friends and associates (past and future) to make enormous profits.
The primary evidence presented by the government for their ‘successful handling’ of the pandemic is always the vaccination programme – which, let us be clear, they have had very little to do with. The vaccines were developed by multinational pharmaceutical companies, at times in collaboration with university research departments, and they were then miraculously rolled out at speed by exhausted and overstretched primary-care staff despite the government’s decade of devastating cuts to the NHS. The development of Covid-19 vaccines, within 12 months of the start of the outbreak, has in many ways been an amazing thing to behold. We now have many vaccinations that are safe and very effective at, if not preventing infection altogether, significantly reducing the risk of serious illness, complications and death. The challenge now is to try and produce new vaccines in time to keep up with the regular development of variants. Unlike with, say, the flu virus, which might undergo annual minor variations, giving enough time to develop effective annual flu vaccines, SARS-CoV-2 tends to pump out new variants, causing multiple outbreaks throughout the year. This means that a vaccine developed to target more recent variants will often be out of date buy the time it is ready for the market.
Currently all the vaccines being given are based on the sequence of the original Covid virus, which was obtained early in 2020 and, as already discussed, are only partially effective at preventing people from getting infected from newer Omicron variants. However, they are thankfully still able to prevent more serious infections in most cases, although there is still a risk for people who have weakened immune systems, for instance. A nightmare scenario would be the development of a variant with the infectiousness of the new Omicron variants, and also the ability to cause serious illness similar to the original SARS-CoV-2 virus, without population immunity.
This brings us back to the absolute and urgent need to start reducing the number of circulating infections – not just in the UK, but globally. The more infections at any one time, the more often SARS-CoV-2 is replicating and the more chance that mutations are taking place. The inability to tackle this is the biggest failure of all in response to the pandemic – largely due to the lack of global cooperation in order to prevent infections worldwide. Vaccines are only available to those who can afford them and this has meant that low-income countries still remain largely unvaccinated. In such states only about 20% of the population have received even a single vaccine, compared to 81% in the rest of the world, and only about 4% have been fully vaccinated (usually two jabs), compared to over 70% in high-income countries.2
Expensive
Vaccines remain expensive and have made the handful of pharmaceutical companies producing them eye-watering profits – Pfizer, BioNTech and Moderna have reportedly made a combined $65,000 per minute in 2021.3 Pfizer received nearly £27 billion from sales of its Covid-19 vaccine last year, making it one of the most lucrative products in history.4
These companies are not going to compromise this profit potential just for the sake of saving lives in countries which cannot afford their product. Hence, they have done whatever they can to block lower-income countries from being able to use the model of their vaccines to manufacture cheaper alternatives locally. Luckily for the pharmaceutical companies, there are international treaties, such as the agreement on Trade-Related Aspects of Intellectual Property Rights, protecting their right to profit at the expense of millions of people’s lives and unacceptable amounts of suffering. This right has been enforced by the world’s higher income countries – none more so than the UK, which aggressively blocked a proposal made in October 2020 by South Africa and India at the World Trade Organization that intellectual property rights on Covid-19 vaccines should be waived for three years.
Of course, this so-called ‘vaccine inequity’ comes as no surprise to us: it is just capitalism doing what it does. The failure to tackle Covid-19 globally speaks of a fundamental systemic failure – an inability to be able to respond effectively to global crises (crises that are created directly or indirectly by capitalism itself). These are coming thick and fast at the moment – whether global pandemics, looming world wars or environmental collapse. Never has it been more imperative for the left to get its act together and for the working class to organise into a force that can vaccinate itself against this pathological system once and for all.
- ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/coronaviruscovid19infectionsurveypilot/15july2022.↩︎
- nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html.↩︎
- int/report/world/pfizer-biontech-and-moderna-making-1000-profit-every-second-while-world-s-poorest.↩︎
- sky.com/story/pfizer-sees-revenues-double-to-81bn-thanks-to-covid-19-vaccine-12536328.↩︎
21/7/22
________
also see:-
Covid-19 and the danger of barbarism – Mohesh Shamanesh, Weekly Worker
Imperialism is responsible for Omicron – Simon Carliner, Left Voice (USA)